I think the masks issue was a bit different. In the past, medicine was practiced without adhering to the scientific method. This is luckily no longer the case. However, medicine has not fully embraced the scientific method but some strange "evidence-based" variant.
During the early stages of the pandemic, high ranking officials suggested we should not use masks because it was not yet "proven" the virus was transmitted via aerosols. And this was a catastrophic decision.
We always need to reason under uncertainty. The correct interpretation of the scientific method would have led to the conclusion that COVID was likely to be transmitted via aerosols (e.g. due to sequence similarity with other coronaviruses, which are known to be transmitted via aerosols) and imposing mandatory masks (because this is a very innocuous intervention).
> During the early stages of the pandemic, high ranking officials suggested we should not use masks because it was not yet "proven" the virus was transmitted via aerosols. And this was a catastrophic decision.
It was criminal. There was a ton of circumstantial evidence: SARS-CoV-1 was thought to spread via airborne droplets, the high rate of transmission, the types of transmission, medical staff infections, reduced rates of transmissions in countries where mask wearing while sick was common, ... we would have convicted COVID19 on less evidence.
But no double blind experiments, so no proof. Go about your day citizens!
It was criminal for way wait too long. If you look at the study of infectious diseases the aerosol transmission model has been discounted for way too long due to inability to “prove” it. If you can’t design an experiment to prove or disprove an idea that doesn’t make it automatically wrong. For example, the aerosol transmission model for influenza was flatly rejected for a long time, even when key scientists found it plausible and had some experimental evidence which wasn’t air tight. In covid’s case the CDC and other experts were grossly exaggerating their confidence that the aerosol transmission model was wrong. My partner was treating covid and in late 2020 after a lot of evidence indicated it was plausible, she still had infectious disease experts make fun of physicians for asking about aerosol transmission. They were grossly confidently incorrect about a theory that had no evidence on either side but had some plausibility (because similar diseases had aerosol transmission). Again, the way the community acted in an area of unknown where it was impossible to prove or disprove was very unscientific.
It was only over a year (with a lot of evidence) that the CDC said “aerosol transmission is maybe sorta kinda possible maybe”.
There are multiple ways to validate an idea, and sometimes you can’t design a blind rct. We know parachutes work despite never having proven it in an rct trial.
> Compared with individuals screened but not enrolled, participants included in the study were on aircraft at significantly lower altitude (mean of 0.6 m for participants v mean of 9146 m for non-participants; P<0.001) and lower velocity (mean of 0 km/h v mean of 800 km/h; P<0.001).
> ... [T]he trial was only able to enroll participants on small stationary aircraft on the ground, suggesting cautious extrapolation to high altitude jumps.
That is by now more than frustrating. Yes, everyone from WHO down to the CDC and there counter-parts in other countries screwed up the mask recommendation. At first, under very difficult circumstances. They corrected that, so, rather quickly. We would all do ourselves a favor and stop bringing this up every single time we talk masks.
...and then someone actually did a cluster RCT for masks and Covid, and found that cloth masks don't have any effect, and surgical masks have a truly minor effect on transmission:
We really need to stop repeating the talking point that "everyone screwed up". The original evidence base was that masks don't do much to stop respiratory illness. "The science" changed in the span of a week in early 2020, based on little more than propaganda. No actual science was ever performed, and once we did some, we found out that the early evidence was pretty much correct.
I find it disturbing that everytime someone points out the actual science of masks (ineffective for stopping viral transmission) they are immediately downvoted or shouted down online.
The cynic in me says that they’re so popular with governments because mask mandates mean that people can wag their fingers and shame the people not wearing masks rather than the politicians who were caught with their trousers down. Masks put the onus on the individual rather than the state for public health, no wonder politicians are loathe to give them up despite patchy evidence for their effectiveness.
It’s also CYA among politicians, and the comforting illusion that you’re doing something. Same part of human nature that leads people to wear lucky charms to ward off evil spirits.
They may mostly be security theatre, but most anti-mask people are exactly as coherent as that guy who gets petulant about removing his shoes at the airport. Still, I don't understand the strong pro-mask sentiment among the vaccinated. Things to add to my shopping list: a face mask proclaiming "hug me, I'm vaccinated".
It's absolutely crucial to distinguish between the different understanding people have of the word masks – cloth masks, gaping-at-the-sides "surgical masks", N95/FFP2 masks, N100/FFP3 masks.
Each random person's picture of masks will be very different from what the next person is thinking.
And it's also very important to distinguish between the different meanings of viral transmission – of what virus, and according to what scientific results it's being talked about.
A lot of the friction comes from this.
In SARS-CoV-2 transmission specifically, I speak about it as airborne or aerosolized, based on all the papers that are out that confirm that now, and I when I say "masks" I tend to think of gaping surgical masks or better, and no, those don't work well enough.
However in the sense of the word masks as N95/FFP2 masks or better—often called respirators—then those masks are almost unreasonably effective at stopping transmission.
Here's the data I base my perspective on, in the nutshell form of some tweets from scientists, tweets linking to scientific papers. (Some are peer-reviewed, some at the preprint stage.)
https://twitter.com/mjb302/status/1409628852867850240 — Important new research examining the real world impact better PPE has on workplace acquired infections of SARS-CoV2. — TL:DR - FFP3 respirators provide 100% protection to healthcare workers looking after patients infected with SARS-CoV2. 1/25
https://twitter.com/andymoz78/status/1441355141051936772 — A thread on our recent pre-print “The removal of airborne SARS-CoV-2 and other microbial bioaerosols by air filtration on COVID-19 surge units” (*Pre-print -not peer reviewed*) — TL:DR Hospital air is dirty, we can clean it
https://twitter.com/DFisman/status/1454776521818886145 — Remarkable new work from Korea shows the extraordinary impact of masks on SARS-2 transmission on public transit. — Parameterized based on *aerosol* simulator. (Because SARS-2 is airborne). Distancing helps, but less important (b/c SARS-2 = airborne).
https://twitter.com/caruzycki/status/1360635674324463616 — 2/ If this disease were only spread by droplets that fell to the ground within 2 metres, [plexiglass barriers] would be a perfectly fine solution to limit transmission. Unfortunately, we unequivocally know that aerosols are important with this disease.
The data for respirators was always better than the data for "masks" (and much better than the non-existent data for "face coverings", whatever those are), but...all of the existing studies of respirators took place in hospitals.
People keep dismissing this, but respirators in hospitals are very different than respirators in the hands of the general public. Fit matters more than anything else, and hospitals have staff and procedures to ensure that PPE is used correctly.
This isn't a small or theoretical concern. Even a tiny gap negates the effect of the respirator, and people don't fit their respirators properly -- in large part because properly worn respirators are annoying and hard to tolerate for long periods of time. I regularly see people walking around with KN95 masks on their faces, with massive gaps around the nose and chin. These masks are pure viral theater.
(Also, not for nothing: two of the twitter links you cite are about respirators in hospitals. the other two are mechanistic studies, which are basically useless. Every failed intervention or drug in the history of medicine has a mountain of plausible mechanistic studies supporting it. Most things don't work, but everything we try has someone claiming that it's a sure-fire solution, based on a lab study.)
One recurring thought I’ve had about the requirement for N95/FFP2 respirators/masks to be closely fitted: Any gap in the seal will drastically reduce efficiency, but a respirator worn in a reasonable manner will always be more efficient than a square mask with enormous high-flow low-resistance gaps on both sides.
In hospitals, high importance is rightfully placed on correctly fitting N95/FFP2 and up – this is so that they function to spec and can be formally assumed to work like the specification indicates so they can be applied as a tool in general use by, well, by a population of staff.
This does not mean that respirators which are worn in a reasonable manner will ever be as poor filtration devices as gaping masks, especially not if the pathogen is airborne / aerosolized and operates almost purely as air flow, not droplets with mass and inertia to consider.
And COVID-19 is airborne and must be considered as airborne. There were five links, and the fifth is a collection of papers :) There is also a significant amount of detail and discussion and framing and context in adjacent tweets i all the links.
If you have any issues with my comment above which is based on clearly delineated and reasonable personal opinion and includes links to the scientific results it is based on, you have a duty to respond, not downvote.
Not gonna defend him, but I was once an atheist and am now Catholic. People do change, and it’s always weird when people pull the “no true Scotsman” card on you. I have plenty of liberal friends who were once conservative.
The sibling comment echoed what I was trying to say. It’s not a no true Scotsman. It’s what the sibling comment said. That’s what I have a problem with. It’s a more and more common occurrence among obviously conservative/right wing people continuously saying they were recently liberal/progressive or are still centrist.
At no point in any blog post did I see the blogger refer to themselves as conservative. Only cheering conservatives on a lot and blaming the left for a bunch of stuff (the only group the blogger said he has identified or belonged to)
You're engaged in tribalism: defining people as members of the other team because they disagree with you on one issue.
I am on the left, and agree with Prasad that the institutional left has done generational damage with its response to Covid, abandoned reason and equity and respect for science. If the "right" happens to agree with me, then that's fine.
A 7 year old child is extremely malleable, and especially socially needs an incredible amount of input to develop as a person. What you do today to a 7 year old for (currently) 2 years has a massive effect later.
Not to mention, how do you think a 7 year olds parents are affected by lockdowns who they are locked up with? Alcoholism? Up. Drug abuse? Up. Domestic abuse? Up.
Think of the children is literally one of the major propaganda tactics the far right has used recently. You can look up save the children sort of stuff. No one doesn’t want to help children. It’s bizarre that Q anon sort of people are able to spin things as if they care about children more than others.
Every one cares about children.
> I’m not sure what makes you right wing
The person consistently bashes the left and praises conservatives. I said that too. Not just school closures in isolation. What would you call someone who does that? Also I brought up the only association they do quickly make is saying they used to be progressive. Another common tactic taken by people who either never were and definitely aren’t now left of center at all. However they will keep leaning right without ever saying they lean right.
A number of political internet personalities in the intellectual dark web continue to do this ploy to varying degrees. Two less egregious examples are Stephen Pinker and Joe Rogan. Two more obviously slanted examples are the Pool and Rubin guy.
—
> Alcoholism? Up. Drug abuse? Up. Domestic abuse? Up.
I stated this in another comment. The status quo has never been good for children who were lower socioeconomically. All metrics: school funding, the amount learned, correlation between exam scores and going to university, all are unfair with our status quo.
Why is there suddenly this behavior of caring for all children as if mostly the right and maybe some centrists who want schools open are the ones who care about children. The blogger specially said the left is bad because they kept schools closed. As if the left doesn’t care about children as much.
All the issues you mentioned effect lower socioeconomic families more than any any other group of people. Where is the care for them when the war on drugs screwed stuff up for so long? It’s hard to believe these things are truly cared about when they have never been a focus for the vast majority of the country, both left and right, until the pandemic became insanely politicize and the right didn’t like the lockdowns.
Your entire argument is, yeah this happens anyway so why do we care.
We care because these things have gotten worse in lockdowns, proven by numbers. Just because something has existed before, doesn’t mean you shouldn’t give a shit when it increases.
Especially if you’re supposedly left wing which I imagine you identify with.
“Poorer people always had more alcoholism and domestic abuse, so why do I care if it goes up if schools close”
That’s a ridiculous attitude.
Btw the whole point of politics and left and right should be that we discuss things and point things out to each other where they are going. Just because that guy to you is right wing doesn’t mean 100% of what he says is wrong. People both on left and right are right about certain things and certain times. That’s why we need debate and not polarization. You are dismissing OP for being right wing in your eyes, and dismissing everything he says.
>He casually says stuff like school closures will haunt society for 100 years
Well maybe you can accuse him of exaggerating but it's true to an extent. In my (third world) country students have effectively missed two years of schooling, I know some primary students who don't know how to read/write very well.
He was referring to the US. the problem is in a number of cases, the most effected groups like minority people[0] with less money, they didn’t want to risk having their child go to school. Those are the groups most effected negatively by distance learning. In that case, what is the blogger fighting for then? If in person schooling started earlier. These kids would be screwed over 10x more staying home while their better off peers go to in person school if school was open in 2020. Which is what he wanted and blamed progressives for messing up.
Since pandemic I have lived in two places: one affluent and the other solidly middle class. Anecdotally, it didn’t seem like any of the children were close to harmed in a generational way. Society already screws over less affluent and colored students their entire lives. It’s interesting that only now the blogger and conservatives care about the well being of these kids’ educations. When otherwise the status quo does not benefit them.
0 the references I’ve seen that I remember are Hispanic and black parents not wanting their kids to go back to in person school.
You should really read the rest of the comments in this thread. People are still asserting masks do "zero" to stop the spread.
Dr. Tam, who is responsible for both gross incompetence AND intentionally misleading the public WRT COVID19, mistakes that literally killed people and, is probably still killing people, remains in her position as Chief Public Health Officer of Canada. This is why I can't let it go.
No, of course not. Because we also continue to listen to people that only were "right" once due to sheer luck that parts of the utter BS they spread turned out to be not completely wrong in a single instance.
On a serious note, how often did they really mess up? In a sense of having consequences that are close to impossible to fix? Not once, if you ask me.
Being once wrong disqualifies then? What I really hate is that some parties have to be right all the time, while others only once. An expert is not the one who is never wrong, but the one who knows why he was wrong and changes his opinion once data and information changes.
Or you had to take one look at the toilet-paper shelf at your local grocery store, leading to the realization that if the same thing were to happen with PPE, it would be apocalyptic.
Not all lies are malicious. Some are necessary. "Masks aren't helpful" was one of those. Everyone with a three-digit IQ should have understood what was really going on, and everyone else was better off believing the lie.
It works well as a name to make people laugh. If they wouldn't laugh, they would cry. This is a good coping mechanism in the face of overwhelming tragedy and suffering.
I works well as a name to remind people that all this was caused by the neglect of the CCP that was instrumental in allowing the virus to spread.
So we are back at blaming China? For what, a couple of weeks delay in locking down Wuhan, a decision by local authorities? China locked down harder and faster than any other country. Heck, they even locked down Wuhan harder when it was still seen as local thing than Germany is locking down, and taking measure against the 4th wave, now.
Blaming China, and one wrong recommendation about masks for the mess parts of the developed world finds itself in is just disingenuous. After Italy was a couple to days to slow in 2020, we know what to do. And we fail doing it. And that failing has nothing whatsoever to do with China or our experts, but rather large swaths of the population, and politicians, refusing to accept measures and guidance.
I see that you brazenly conflate the country with the party in an attempt befuddle HN readers, but that does not work. They are not tricked that easily.
No, we are back to where we started, placing blame where it belongs, on the CCP: first for suppressing the information about a new SARS outbreak and claiming it was not human transmissable, then second for a laughably ineffective Wuhan lockdown. It was ineffective, allowing asymptomatic infected people to escape, for two reasons:
• Some people who did not fancy being put under lockdown left the region by car and found holes in the secure perimeter or simply bribed the patrols, those who were successful doing so shared the routes and bragged about it on Wechat.
• The party secretariat ordered the airport to stop domestic flights, but the international flights continued as usual. Tracing revealed the virus was subsequently carried off abroad, initially to Thailand.
I'm not conflating anything. When it come to pandemic counter-measures, the country and the government (in one party systems, the party) are and can be used synonymously.
But let's say, just for a thought experiment, it was all the CCPs (bad communists, aren't they?) fault. How exactly does that help us now? Or does it excuse some of our democratic governments from screwing up? Or people from not getting vaccinated? I don't think so.
Yeah, the CCP sucks. Taking away personal freedom, incerting spyware in phones in other countries, ignoring human rights left and right wherever they go, paying of our capitalism based democracies, continuously threatening Taiwan and strong-arming everyone (from the IOSB all the way to western democratic governments) from acknowledging Taiwan as an independent nation. But COVID? Not so much.
Yes, you are, as you admit to it with the next sentence. I have read your argument why it should be okay and understand it, but I cannot allow you to be less than precise with your writing. When we examine the (in)actions of the party, we should name the party, or talk about the government. We should not use the term for the country because that concept also subsumes the territory and the people. The people as a whole however cannot be held responsible for the government because most of them neither support it (in the sense that if they could magically wish it away tomorrow free of consequences, they would do so) nor did they vote for it or bring it into power nor are the interests of the government and the interests of the people aligned or represented.
Talking about the country or the people as a way to deflect from the party is an old propaganda trick employed on a daily basis by the party, it must always be challenged.
> bad communists, aren't they?
What's the point of that tangent? Everyone knows there is not much communism left, the reforms after Deng have completely abolished the concept in its economic interpretation. The word itself, the trappings of hammer and sickle, the raised fist during a vow, this is all but for show. The most ardent adherents to the ideology can nowhere be seen in positions of power, that's mostly found among block wardens who have a genuine interest in helping out their neighbours and sharing among the local community and also the members of the youth organisations because young minds are easily impressionable by the theory.
If I would characterise the CCP as it relates to the outward world, words like deliberate liars and cry-bullies, incredible neglect and delinquency of duty, not giving a shit about human dignity or life, destroyers of the environment come to my mind first, rather than communist.
> How exactly does that help us now?
It helps by changing our mind in the light of information. We will not be blind-sided any more by information that turns out to be manufactured or false, we will be more cautious and we can make better decisions that way in the future. To make this more clear: instead of operating on a baseline of medium to high trust as it is has developed as the common case in our Western high culture over the last centuries, we recognise that the trust has been abused and operate from a baseline of low trust instead.
> does it excuse some of our democratic governments from screwing up?
Yes, I think somewhat. They are a victim of disinformation. I keep a large share of the blame on our governments because they are more interested in stocking water cannon lorries and police APC rather than masks and other disaster supplies.
> Or people from not getting vaccinated?
IMO that is not in the purview of any government, in the sense that they should offer vaccination free of charge to any resident, but not enforce ("accept vaccination or face repression by the power of the state") or even nudge ("accept vaccination and receive a yellow pass or face not being able to participate in social life any more"). I have thought about this and have come to the conclusion that any amount of force is a human rights violation on medical ethics grounds. This should be an explicit part of the human rights declaration, but sadly is not.
I am vaccinated, I personally encourage the people near me to get vaccinated, and demand that those who refuse on non-medical grounds must take responsibility for the consequences of their choice and when getting sick go into a forest to die and not take up a hospital slot because it is not fair to earn the benefits of being part of society without paying the dues.
> But COVID? Not so much.
I don't get it, you enumerate five items of suck, but the spread of the virus through neglect and disinformation which falls into the same observable operative patterns of the party will not be a part of it?
There are hundreds of studies. And, it’s pretty conclusive that masks have zero efficacy for stopping viral transmission. But, you’ll get shouted down by the mob for pointing this out. Nobody reads the actual studies.
but based on your own contention, you won't read it, so here's a key sentence from the abstract:
The preponderance of evidence indicates that mask wearing reduces transmissibility per contact by reducing transmission of infected respiratory particles in both laboratory and clinical contexts.
> There are hundreds of studies. And, it’s pretty conclusive that masks have zero efficacy for stopping viral transmission
Could you link some?
What I have read seems to suggest otherwise, for example "Efficacy of face mask in preventing respiratory virus transmission: A systematic review and meta-analysis" [1]
Key conclusion: "Meta-analyses suggest that mask use provided a significant protective effect"
And at this point, nearly 2 years into the pandemic, claiming that cloth masks do nothing is not arguing in good faith.
A number of studies have been linked in sibling comments, studying the effects of cloth masks. They work to significant reduce exhaled contaminant load.
> In one study, during talking, unmasked subjects expelled more than 5,000 contaminants per 5 cubic feet; 7.2% of the contaminants were associated with particles less than 4 μm in diameter (68). Cloth-masked subjects expelled an average of 19 contaminants per 5 cubic feet; 63% were less than 4 μm in diameter. So overall, over 99% of contaminants were filtered. The second study used the same experimental setup, but studied a wider range of mask designs, including a four-ply cotton mask. For each mask design, over 97% contaminant filtration was observed (69).
Also, at this point we know that even if you catch COVID-19, the viral load that you catch plays a factor in how seriously ill you get. Masks reduce the viral load that a sick person exposes others to.
>> Conflating N95 respirators with masks indicates you are not arguing in good faith
Why?
I am not the parent and also not a native English speaker - is it not common to call respirators also "masks"? Does that term refer to surgical masks only? I live in the Czech Republic and the Czech word "maska", which is translated as "mask" (and I assume comes from the same latin origin) is pretty general term used to refer to basically anything that covers something.
If it is not a general term, do people in the US still really use surgical masks with the intention of protecting themselves from Covid? Where I live we would be talking about FFP2 and above, discussing surgical masks as covid protection would be irrelevant because no one wears them (granted, many people do not wear anything). Is it not like that in the US?
Late to reply, but yes. I'm a native English speaker, and everyone I know refers to N95 masks as masks. I don't know a single person who refers to them as respirators, even though that's the technical term.
Fortunately there was never any possibility of welding NY Metro area residents into their apartment as a reaction to COVID, like what happened in China.
Only after CNY, the super-spread event that turned this global.
What is especially galling is that for all his hardline rhetoric and complete lack of respect or fear for the rest of the world Xi is terrified of the reprisals at home if he banned CNY travel.
Are you referring to the insanity of the last New York administration that was responsible for this https://en.wikipedia.org/wiki/New_York_COVID-19_nursing_home... and measures including not putting infectious people into nursing homes? If not, what are you referring to and what key early measures do you think should have been taken?
We as a society don't want administrators adhere to the scientific method. We want them to be conservative.
For some reason, people don't see the consequences of action and inaction symmetrically. If an administrator chooses a risky intervention and it turns out to be the wrong choice, we hold that person more liable than another administrator who chooses inaction with equally bad consequences. Because we give administrators power and hold them liable for their choices, we expect them to avoid risky interventions out of self-interest.
Early in the pandemic, experts put too much weight on the risks of improper mask use. Perhaps because they were trained to use masks in risky situations where the consequences of improper use were real. It took them some time to realize that the general public would be using masks in low-risk situations, which reduced the expected risks significantly.
> For some reason, people don't see the consequences of action and inaction symmetrically.
Prevention paradox.
Regarding the masks, at least in Germany the problem was different... politicians knew that masks were effective but, since the stockpiles of the Cold War era had been dismantled and domestic production all but non-existent because no matter what China is going to be at least 10x cheaper, they feared a "bank run" on the few masks that were still in the country.
Politicians didn't have the guts to come out and say "yes, we know that masks help, but please don't go on shopping sprees, we need every single mask there is for the hospitals".
France also did that, except it was not cold-war era: after the 2006 bird flu scare, the country decided to set up a strategic reserve, which obviously required domestic production which would go towards stockpile upkeep so there would be companies ready in case of need.
In 2009 as H1N1 started ramping up the reserve had half a billion masks (and 100 million already ordered), the health minister launched buildup order to increase the stockpile to 1.7 billion (a billion surgigals and 700m N95/FFP2).
After H1N1 drew down, the health minister got greatly criticised for the expense, and following the event the agency got slowly starved out: the government decided to drop FFP2s entirely, and significantly draw down the stock of surgicals. In 2013 it moved the entire thing over to private entities (companies were supposed to stock up masks for employees, imagine how stupid that idea is).
Obviously this completely killed the domestic production in short order as companies were not doing jack shit, and even if they had they’d have bought chinese production. As soon as 2015 all the companies set up after 2006 had folded, and domestic production capabilities were essentially gone.
In 2016, the agency which had been specifically set up to oversee pandemic preparation and response to pandemics was killed, officially “folded” into a more general public health agency, after having been slowly starved of funds for years.
When COVID-19 hit, the country had no production capabilities (500 million masks a year) and the stock was essentially nil (about 150 million masks, 3 weeks worth of healthcare demand alone).
This was particularly maddening because, technically, they were right about it not being "airborne". By definition it wasn't "airborne". Unfortunately the definition of "airborne" was completely nonsensical.
"Airborne" required the droplets to be below a certain size, when that clearly had nothing to do with whether or not it travelled long distances through the air. It took a lot of frustrating work by scientists who knew what the hell they were talking about to convince the high ranking officials to stop killing people.
This echos my partner’s experience (the treat covid in an icu). This was almost a year un with some plausible evidence and several countries saying they thought aerosol transmission was likely. Yet the key agencies and experts here were aggressively saying aerosol transmission was very unlikely.
That logic works on the assumption of science and cooperation that we are all telling each other the truth so that everyone may benefit.
I posit that's not what happened, there was no absent evidence. The NHC knew full well that they had (another) SARS on their hands in January 2020, but lied to the WHO because they were directed by the party to suppress the findings for the usual reasons (don't rock the boat, save face on the global stage, keep the populace under control). The WHO took this false information and neglected to verify it before disseminating it, so they are complicit in the affair.
People try to convince me that "nobody could have known masks were effective for respiratory illness until the science came in" like the doctor's office didn't have surgical masks specifically for people with flu-like illness well before anybody had ever heard of COVID-19.
Masks have been heavily studied re viral transmission and been show to have zero effect. It’s like people are ignoring the giant body of prior scientific research. Masks aren’t a new idea in medicine.
Also note, what you posted is not a scientific study. It’s a made up model. Real world evidence is falling in line with previous scientific knowledge. Countries w/out mask mandates have no statistical difference in transmission, as expected. But, the whole thing has been politicized.
Even that study believes that good masks help:"We did not consider the use of respirators in the community. Respirators are tight-fitting masks that can protect the wearer from fine particles (37) and should provide better protection against influenza virus exposures when properly worn because of higher filtration efficiency."
The same metastudy says hand washing isn’t statistically significant in stopping pandemic flu spread, but is careful to note that doesn’t mean it’s ok not to wash your hands. There are many other diseases which are prevented by washing your hands.
Generalizing from influenza to COVID-19 seems like a big assumption.
"A similar survey by Nature on 1,576 researchers who took a brief online questionnaire on reproducibility showed that more than 70% of researchers have tried and failed to reproduce another scientist's experiments, and more than half have failed to reproduce their own experiments."
Not to mention that basically all studies are paid for by one of only 3 (connected) sources - military, government or corporations.
If you control the purse strings, you decide what to (or not to) study.
Which explains all sorts of basic 'anomalies' - such as that we don't know what the best sort of diet is for us.
>Which explains all sorts of basic 'anomalies' - such as that we don't know what the best sort of diet is for us.
It took way too long to figure out that absolute LDL cholesterol levels predict nothing and that only oxidized LDL (even at extremely small concentrations) is a predictor for heart disease.
And unfortunately, due to politics, we have (in the USA) half the nation thinking that the top health and government officials were/are wrong about absolutely everything (including vaccines), and the other half of the nation thinks that the top officials got everything exactly right (and refuse to question what could have been handled better).
So California looks at Florida in horror, even though COVID just keeps on truckin' through Cali. And Florida screams that a mask is history's greatest threat to liberty, even though it's a plain and obvious way to reduce transmission.
> So California looks at Florida in horror, even though COVID just keeps on truckin' through Cali.
California’s recent COVID death rate per 100K population is 2/3 Floridas, and the COVID incidence is concentrated in the counties with Florida-like attitudes.
> Now adjust for risk based on population age differences and see how the difference between states looks.
About what you’d expect if the actual recent infection rates were similar after Florida's drop from its mich higher recent peak, rather than Florida's being now much lower the way the reported case rates would suggest.
> even though COVID just keeps on truckin' through Cali
California’s death rate is far lower than Florida. This isn’t something you should be both-sidesing. Tens of thousands of Californians are still alive because of the measures we’ve taken.
And it’s not so much horror as disgust and confusion, like seeing someone smearing feces on themselves and saying “I trolled u!!”
Maybe I expressed myself incorrectly, because my goal wasn't to "both-sides" this. My point was that there is a complete refusal (as far as I see) to do a critical evaluation of the steps California took, to see whether they were excessive/broad (or, I suppose, too relaxed) in some circumstances. To even ask the question, as I'm doing, puts you in the false-equivalence crosshairs.
Hmm, I disagree it’s not being debated here. There’s certainly a lot of healthy debate. It just happens to be centered far more towards the “principle of boosting the disadvantaged” (so our concern over the immuno-compromised, the infirm and weak, the underprivileged, etc), whereas the debate elsewhere kind of sidelines them, or at least puts the concerns of healthy privileged people at the same level.
Not sure my point is getting across. I’m not quite sure what my point is. Still trying to figure out what makes California (and especially San Francisco) different without resorting to simple left vs right language.
And if California had the same death rate as Florida, there'd be an additional 40k dead people. These things aren't remotely symmetrical and it's such a disservice to pretend like "both sides are bad".
If you re-read my post above though, I'm not saying they're symmetrical. But to me it's striking that one state put in severe restrictions on business/etc for over a year, and the other state just pretended there was no pandemic, and yet California's did not even halve the case/death rates compared to Florida (per capita).
So the question California dares not ask itself is: were all the restrictions actually necessary? Maybe small businesses could have been allowed to open sooner with a mask + ventilation requirement, for example. Or maybe a single, uniform policy did not make sense for the enormously-varied state. But you can't ask those questions.
If you look at California on a county-by-county basis the restrictions definitely did halve the death rate (and beyond). The counties in California that behaved more like Florida were rewarded with a great deal more death. San Francisco, which had not only tough restrictions but high compliance, had the lowest Covid-19 death rate of any metro in the country.
You needn't use your real name, of course, but for HN to be a community, users need some identity for other users to relate to. Otherwise we may as well have no usernames and no community, and that would be a different kind of forum. https://hn.algolia.com/?sort=byDate&dateRange=all&type=comme...
Also: please make your substantive points without flamebait. Your comment here would be fine without the last sentence.
I don't think China had any preference on whether the world was going to wear masks. Let's not vilify them too much. This has nothing to do with the origin of the virus which is the only topic that seems to make them touchy.
I think it's more that they were suggesting that an aggressive response to COVID19 would have appeared to be an anti-China move, and thus further jeopardize the US relationship with China.
I disagree. We knew masks would help, and medical professionals were using them.
Basically I kept hearing only n95 I’d effective, or you’ll use them wrong. We know masks would help more with larger droplets, yet we persisted with the lie.
That played into their thinking, according to what officials like Fauci have said later in interviews. They didn't want to encourage people to just buy up scarce masks. But if you ask me this was extremely shortsighted because turning it into a controversial political football was the worst thing that could have happened.
They could have simply told people "masks are good, but please leave them to health worker", i.e. appeal to people's better side. Instead they chose to take people for idiots and lie to them, and lo and behold, people don't like being lied to and taken for idiots.
This was not just in the US, exact same thing happened in most of Europe.
Given what that qanonsense manages to turn the least controversial things into political football, and doesn't care for whether or not there are any facts backing their position, it wouldn't have mattered. Republicans would have just started complaining about it in March, instead of whichever later date the CDC changed their guidance.
The first rule of politics is to never let a good crisis go to waste. The second rule of politics is to always piss on whatever your opponents are doing, regardless of whether it makes sense or not.
Great point about Qanon and facts not being necessary. The fact we keep having the same argument on HN about masks is proof that it doesn’t really matter what Fauci did back then. It’s just weak justification for current bad behavior.
If they were more decisive they could have avoided it becoming a partisan issue in the first place. There was nothing foreordained about it being an issue at all. Even if I’m wrong about that, they did harm to the people who listened to their advice.
There weren’t enough masks for health care workers at the time and we were facing a possible meltdown of the entire health care industry (and societal meltdown). Advising people not to hoard masks, and instead leave them for health care workers, was probably the right move. Even if our government said “go get masked up” nothing would’ve changed, as proper masks were out of stock for months.
I’m not saying the deception was necessary, just illustrating it’s not black and white. It would’ve become a partisan issue regardless with Trump doing his performative masculinity routine and refusing to wear them.
But the deception is specifically what I'm objecting to. Yes, it would have been quite reasonable to say "healthcare workers need the masks -- please leave them for them." By doing a public volte-face, the medical authorities opened the door to questioning of their advice and the "macho posturing" that you're talking about. I'm not convinced that it would have played out the same if they hadn't made such a foolish decision.
> medicine has not fully embraced the scientific method but some strange "evidence-based" variant.
Why would you not want to follow a conservative, evidence-based variant of the scientific method?
> During the early stages of the pandemic, high ranking officials suggested we should not use masks because it was not yet "proven" the virus was transmitted via aerosols. And this was a catastrophic decision.
And the current administration continues to employ this official and give them a microphone
Because apparently they are too dumb to evaluate low risk-low cost interventions like wearing a mask in a different way from high risk-high cost interventions like taking a new drug.
What happens when different people perceive the cost of these measures differently though?
That's half the problem here, with anti-maskers screaming that they can't breathe.
You can try forcing them, like we're doing now, and they'll just take off their mask to cough and sneeze like half the passengers in my last flight + take every possible option to take it off + wear it off their nose to begin with.
The masks issue is different because we have very little actual evidence that masks in the hands of the general public have a substantial effect. The best evidence out there suggests a small impact (~11%) for surgical masks in an unvaccinated population, and none for cloth masks [1]
The evidence quality is roughly as poor as that for ivermectin, vitamin D, etc., except that it has become a wildly political issue, fraught with propaganda to the point that most people will vehemently insist that the evidence quality is higher than it is. It is therefore deeply ironic that Slate is arguing about risk compensation, while using NPIs as an example of the kind of safety behavior being deterred by discussions of risk compensation. Did any of those NPIs do anything at all? We never did proper randomized studies, so we really have no idea.
This feels like so much more propaganda: one side said that risk compensation is a thing, so now we must attack the notion, to ensure that $MY_PREFERRED_INTERVENTION is properly imposed on society. But nobody much cares if the intervention works...
The masks are secondary to the issue of refusing to acknowledge the high probability of airborne transmission.
People were washing their hands, using hand sanitizer, opening doors with crazy key-chains, basically not touching anything, wearing gloves, fist and elbow bumping ... when they really needed to not be breathing each others air.
Yeah, that was definitely part of it too. It was plausible for a minute there that surface transmission was real, but then it took way too long for the CDC and the WHO to admit it. So now, even today, I see people wearing dirty rubber gloves in the grocery store (sigh).
There's simply no part of this pandemic that makes "the experts" look good, and it has utterly destroyed any remaining faith that I had in journalism. Now we merely have competing ideological factions, and their preferred sources of propaganda.
>So now, even today, I see people wearing dirty rubber gloves in the grocery store (sigh).
A month ago, I was judgemental towards a couple who were "overly protective" about the virus. It turns out they did REALLY risky stuff, and they were "overly protective" to protect me.
Maybe the people in the grocery store with gloves have open wounds and don't want to spread infected blood around.
Or maybe they're just average people, terrified out of their wits by a narrative that wasn't based in facts, and was promulgated by a media industry that needs panic to survive.
I guess we'll never know. But there sure are a lot of folks wearing gloves now who weren't wearing them before. And that's why I was sighing.
Yeah, it's totally the fault of the CDC that people continue to do things that don't make sense. Totally a top down problem, all they had to do was get the messaging right and no one would have done anything wildly incoherent for the entire pandemic.
If the CDC and the WHO and "the experts" hadn't spent months flooding the airwaves with the message that people should be scared of fomites, while ignoring aerosols?
> There's simply no part of this pandemic that makes "the experts" look good, and it has utterly destroyed any remaining faith that I had in journalism.
Yeah, the inability to call the "experts" out when they were clearly wrong and now the constant interviews with "the vaccine hesitant" ...
11% (just adopting the number from your comment, no idea if that is the real figure) is huge. It would turn a spread 1.05 into one of 0.94 assuming that number has a direct impact like that. That's the difference between 'out of control' and 'decreasing to the point where we can start doing contact tracing'.
That's exactly what is wrong with all these discussions, the cost of wearing a mask is negligible compared the potential cost of not wearing a mask: so wear a mask. It doesn't matter if it is proven to help yet or not, the fact that it may help and won't harm is the only thing that matters when deciding whether or not you should wear one.
As for the rest of your comment, the evidence quality for Ivermectin is substantially lower than that, so low that it drowns in the noise and is essentially a complete wash, and there are substantial downsides to using it in quantity.
> 11% (just adopting the number from your comment, no idea if that is the real figure) is huge. It would turn a spread 1.05 into one of 0.94 assuming that number has a direct impact like that.
No, because that's not what the 11% number was measuring. You can't just take an 11% relative reduction in population seroprevalence at a given time, and then blindly multiply the virus R0 by that factor. They observed a drop in symptomatic seroprevalence that corresponded to about 1 case for for every 1300 people who wore a mask. That is nowhere near an 11% drop in R0 (which you'll recall is an exponent).
> That's exactly what is wrong with all these discussions, the cost of wearing a mask is negligible compared the potential cost of not wearing a mask:
How do you know? Have you measured it? No, of course you haven't. You're just asserting things.
> so wear a mask. It doesn't matter if it is proven to help yet or not, the fact that it may help and won't harm is the only thing that matters when deciding whether or not you should wear one.
Fine. You should take Ivermectin, then. And vitamin D. And flush your sinuses daily with a neti pot. And get your chakra aligned. It's essentially the same argument. Can't hurt, might help! By your logic, it all must be done.
...or do you just pick-and-choose which unsupported interventions you prefer to believe in?
(for the record: I do not believe you should take Ivermectin. But it is the same argument.)
> the evidence quality for Ivermectin is substantially lower than that,
It really isn't. Just like mask studies, there are a few weakly suggestive good ones, and a few bad ones that make ridiculous claims, and a whole lot of nonsense in between.
> there are substantial downsides to using it in quantity.
No, not really. It's a pretty common, safe drug. We probably know more about the downsides of Ivermectin than we do about the downsides of (say) masking young children in school.
You are arguing the letter and not the intent, as you've done in many of these threads before.
You are also continuously seeking reasons to justify the way you have already decided you want to go about this, so effectively you are just arguing for your own satisfaction, not to gain insight.
Your arguments by assertion hold no water for me. Good luck with this attitude.
No, he's not. Ivermectin is one of the safest drugs on the planet. As evidence was emerging that in some studies it MIGHT work, people should have been taking it, just like masks. Because why not? Risks are low, and it might work.
If you are arguing anything else than you aren't actually being consistent in your reasoning.
It is, but it isn't going to work against COVID, period. That people take it is their problem, the only study that showed actual anti-viral effects was at several times the recommended dose for people and that was in vitro.
Risks are also low for eating 50 Kg of bananas, it might cure COVID, so why not try it? This sort of reasoning is complete nonsense when it comes to picking your medications.
The null hypothesis is "it does not work". Then you carefully design a study to take care of all the variables, you do your double blind test with a placebo and you look at outcomes. That's the standard. Anything less simply won't do. 'Might work' isn't a reason for (self) prescription.
As for mask effectiveness: they work, there is ongoing debate over how much they work. Like everything else in terms of countermeasures, absolutely nothing will be a 100% sure filter so we layer multiple filters on top of each other to improve the degree of protection we achieve, aka the cheese model.
> It is, but it isn't going to work against COVID, period.
It's interesting how you say that so definitively, when there are multiple, large RCTs ongoing, evaluating the question.
Perhaps you're substituting your opinions for science?
> The null hypothesis is "it does not work". Then you carefully design a study to take care of all the variables, you do your double blind test with a placebo and you look at outcomes. That's the standard.
> As for mask effectiveness: they work, there is ongoing debate over how much they work.
Funny how "the standard" shifts from topic to topic, sentence to sentence. When it's an intervention you support, the presumption is positive, even if the collective evidence of effect is...mixed, at best.
if it works it isn't going to work to the degree that has been claimed so far because an effect that big would have been easily observed.
So these studies are in the realm of 'we can't rule it out 100% let's check one more time'. Since this is a forum and not a scientific paper I can claim with some confidence that it isn't going to work, if you want to take the opposite side of that bet be my guest.
Masks work, whether it is 10% or 15% effective is what's at stake there, not whether they work or not. If ivermectin was 10% effective it would have been established long ago.
You are guilty of exactly those things that you accuse me of.
No, I'm just done with the bullshit. I even qualified my statement to ensure that it was clear that I just used the 11% as a means to show why no matter what the difference is it can make the balance shift from growing to shrinking.
Somehow I start to suspect that masks might have a similar effectiveness that are dependant on climate, air humidity and widespread co-infections. Maybe not effective against covid but might prevent other infections that ultimately make covid worse or make them more susceptible to covid.
I'm generally in support of the masking rules BUT I also have a very young baby and there is definitely a high cost for him. Not seeing a smile when he is left at daycare has caused him to cry more than once, I don't even want to think about the long term effects of seeing so much less facial expression in his critical first months.
I know this is a talking point of anti-maskers but let's not pretend all of the other side's arguments are bogus _because_ they made it. This is just one example, there _is_ a cost to masking up the entire population.
Vinay does a big disservice to that 53% number and is in my opinion, extraordinarily dishonest about the 10% number.
He says;
> Interestingly, in the only published cluster RCT to date during COVID19, surgical masks had an 11% risk reduction and cloth masks had no effect at all on the primary endpoint of symptom driven lab positive result
The actual study showed that with intervention, the scientists increased the rate of mask wearing from 13% to 42% -- and that 29/100 person uptake was enough to reduce Covid seropresence by 11% in the community. That's a huge effect! Fewer than half of the people in the villages were wearing masks and symptomatic Covid saw >10% reduction compared to villages without extra mask wearing. It's abundantly clear that the effect would be far greater with universal masking so to say "mask wearing only leads to a 10% reduction" omits a massive part of the story.
To quote the authors who tried in vain to prevent people like Vinay from mangling their research:
> Our results should not be taken to imply that masks can prevent only 10% of COVID-19 cases, let alone 10% of COVID-19 mortality. Our intervention induced 29 more people out of every 100 to wear masks, with 42% of people wearing masks in total. The total impact with near universal masking–perhaps achievable with alternative strategies or stricter enforcement–may be several times larger than our 10% estimate. Additionally, the intervention reduced symptomatic seroprevalence more when surgical masks were used, and even more for the highest-risk individuals in our sample (23% for ages 50-60 and 35% for ages 60+). These numbers likely give a better sense of the impact of our intervention on severe morbidity and mortality, since most of the disease
burden is borne by the elderly. Where achievable, universal mask adoption is likely to have still larger impacts.
> The actual study showed that with intervention, the scientists increased the rate of mask wearing from 13% to 42% -- and that 29/100 person uptake was enough to reduce Covid seropresence by 11% in the community. That's a huge effect!
No, it isn't. Because he's being generous: the 11% difference was on a baseline seroprevalence of 0.76%. So you have a study where cloth masks were shown to be completely ineffective, and the total absolute effect size of the surgical mask arm was .08% (edit: 0.09% per the numbers in the paper).
In other words: you'd have to get 1300 people to wear masks to prevent one seropositive (in case you're wondering, the confidence interval on that value overlaps zero.) No matter how you spin it, this is a small, small effect. And this is in a completely unvaccinated population -- the best possible scenario for masks.
Even if we accept the argument that "several times more" people would be protected if we lived in a fictional, ideal universe where everyone wore surgical masks (newsflash: we don't), we're still only talking about a total effect size of a fraction of a percent.
Oh and by the way, it's particularly hilarious that the paragraph you quoted says the following:
> Additionally, the intervention reduced symptomatic seroprevalence more when surgical masks were used
That has to go in my top-five lifetime examples of weasel-wording for reframing negative experimental outcomes. Cloth masks showed no effect. Saying that surgical masks reduced prevalence "more" is like saying that together, Ootani Shohei and I hit 46 home runs last year. But yeah, he hit more.
> Because he's being generous: the 11% difference was on a baseline seroprevalence of 0.76%.
Wait a second.
> In other words: you'd have to get 1300 people to wear masks to prevent one seropositive (in case you're wondering, the confidence interval on that value overlaps zero.)
You are assuming 0.76% prevalence. This is, I assume, in specific point of time, but somehow, you extend this to long-term intervention.
If you spin COVID-19 "but only 0.5% of population is infected _right now_", any intervention will seem extremely ineffective. "Oh, you want to vaccinate 300 millions of people to prevent 2000 deaths" (without saying it's 2000 deaths _per day_).
I am not. I'm using the numbers from the paper to illustrate a point.
Even if seroprevalence was as high as 6% at any given time (which is about as high as it ever was in NYC, for example), an 11% difference is 0.66%, or 1 case per 152 people wearing masks. And that's in a fully unvaccinated population.
We're simply not talking about huge differences here. Certainly nothing close to a statistically meaningful difference in R0.
To be fair, it's not necessarily the case that an unvaccinated population is the best case for masks. If vaccination reduces infectiousness, adding a mask on top could push a small exposure down to a noninfection, whereas a one-time large exposure would overwhelm it.
> In other words: you'd have to get 1300 people to wear masks to prevent one seropositive. (Oh, and by the way? The confidence interval on that overlaps zero.)
That's not accurate unless I'm missing something... sticking with just the surgical mask arm -- the effect size of 0.08% was based on a binary mask vs. non-mask intervention. It has no relation to the number of people masking. The intervention was getting more people to mask -- they succeeded mildly, where 6/10 people still hadn't masked. But that was sufficient for a 10% reduction in seropositive cases.
Edit;
They actually address this specifically;
Our estimates suggest that mask-wearing increased by 28.8 percentage points, corresponding to an estimated 51,347 additional adults wearing masks in intervention villages, and this effect was persistent even after active mask promotion was discontinued. The intervention led to a 9.3% reduction in symptomatic SARS-CoV-2 seroprevalence (which corresponds to a 103 fewer symptomatic seropositives) and an 11.9% reduction in the prevalence of COVID-like symptoms, corresponding to 1,587 fewer people reporting these symptoms.
So for 51,000 people additional people wearing masks -- 1,600 people were spared Covid symptoms and 103 people were spared symptoms + seropostive diagnosis. This with only a total of 42% of people wearing masks and a relatively low level of underlying Covid.
It's an especially obvious intervention based on the exponential potential of Covid infection and early R0 of 6 or whatever it was, plus how effective the surgical masks were (especially in older age groups via Figure 3).
> That's not accurate unless I'm missing something... sticking with just the surgical mask arm -- the effect size of 0.08% was based on a binary mask vs. non-mask intervention.
The RCT was a binary test of each kind of mask. Any other outcome is imaginary. There's no mathematical adjustment that can tell you what would have happened in the hypothetical alternative universe where everyone wore a surgical mask. That's just storytelling with numbers.
> But that was sufficient for a 10% reduction in seropositive cases.
No. It was a an 11% relative reduction, on a 0.76% seropositivity rate. The actual effect size was about 0.09% (I wrote 0.08% earlier, because I just divided the two numbers, and didn't use the figures from the paper). When you compare the cost of an intervention to the benefits, you use the absolute effect size, because you don't pay relative costs for your interventions (e.g. is it worth forcing every toddler in the world to wear a mask while sleeping for a "huge" 66% relative risk reduction from 0.0000003% to 0.0000001%? Probably not unless you're a crazy person. The costs vastly outweigh the benefits, even though the "relative" benefit is strong.)
> Our estimates suggest that mask-wearing increased by 28.8 percentage points, corresponding to an estimated 51,347 additional adults wearing masks in intervention villages, and this effect was persistent even after active mask promotion was discontinued. The intervention led to a 9.3% reduction in symptomatic SARS-CoV-2 seroprevalence (which corresponds to a 103 fewer symptomatic seropositives) and an 11.9% reduction in the prevalence of COVID-like symptoms, corresponding to 1,587 fewer people reporting these symptoms.
This is garbage. They're combining the two mask arms and claiming a combined effect size, even though the cloth mask arm was shown to have no effect. You can't do that. They're spinning like crazy to hide a weak outcome. They also don't report the raw numbers for the arms, and they don't dwell too much on the fact that "distancing" increased in the mask villages over the controls. That could easily swamp the measured effects. But I digress.
The surgical mask villages had 106,201 people, and an 11.2% relative reduction in seroprevalence, from 0.76% to 0.67%. The cloth mask villages saw essentially no difference at all: 0.76% vs 0.74%
There's simply no way to look at this data as anything than incredibly weak evidence for masks. I honestly can't believe we're fighting about something that makes, at best, a tiny fraction of a percent difference in outcome. Mass hysteria.
> I honestly can't believe we're fighting about something that makes, at best, a tiny fraction of a percent difference in outcome. Mass hysteria.
I whole-heartedly don't understand this.. in the places with universal masking, there is essentially no Covid (most of Asia, even cities like SF). Surgical masks are obviously sufficient to prevent most infection in hospital and other clinical settings. There's evidence that even a small portion of people wearing them in public reduces the incidence of disease. And your takeaway is that it's mass hysteria to encourage an extraordinarily cheap NPI?
> in the places with universal masking, there is essentially no Covid (most of Asia, even cities like SF).
Just completely, utterly wrong. Japan had a huge spike this winter. Korea is currently at all-time highs. Vietnam is currently near all-time highs. Thailand peaked at 20,000 cases per day, and is currently at 10,000.
These numbers are lower than the US in absolute terms, but claiming "essentially no Covid" means only that you aren't informed of the reality of the situation. Covid is running rampant across Asia, even now.
> There's evidence that even a small portion of people wearing them in public reduces the incidence of disease.
There is literally no evidence of this. The few RCTs that have performed suggest the opposite: you have to put masks on a huge number of people (hundreds to thousands) to prevent even a single case.
> And your takeaway is that it's mass hysteria to encourage an extraordinarily cheap NPI?
No, my takeaway is that there's very little evidence supporting the use of masks. Because there isn't. And most of what there is, is of exceptionally low quality.
Spike in Japan this winter? lol ... yes it's really scary here 73 cases a day nation wide. The only spikes came during summer due to Olympics and Paralympics. Please stop making stuff up.
The major difference to Germany I see between the two countries in terms of measures, Japanese were masks (vaccinated) and Mask Wearing in Germany has become political as it did in the US.
it's dismaying to see a reasoned (if countervailing) position being so reflexively suppressed, and maddening to witness the mass hysteria still buttressing ineffective mandated interventions like public masking.
the only places outside of healthcare settings where masking plausibly makes any difference for ordinary folks is at home (amongst friends/family) and in crowded indoor social gatherings (club, house party, etc.). a modicum of physical distancing is all that's need in most public places to minimize tranmission risk about as much as is possible. combine that with masking public-facing workers (like cashiers), and we've maxed out the potential of masking as an intervention. everything else is theater.
Striking that the only reply in this thread which refers to actual data is the one which is downvoted. More than a political issue, for many, mask-wearing has taken on something like religious significance.
Does it? It's a link to a Substack article with some numbers, but no actual data. Not even the links or names of the papers and articles. At first I thought it was a stylistic choice, but the author does link his own whitepaper from the Cato institute.
There's also a thought experiment, which is convenient, since the outcome is open to everyone's interpretation. But it's not actual data.
if you are getting your medical information from a substack page, I don't think anything anyone here will convince you otherwise...
pointing out elsewhere in the thread that when the CDC fucked up, they ultimately admitted it and changed recommendations, does not support your argument.
If this pandemic has proven anything at all, it's that incompetent and/or corrupt doctors are a dime a dozen. Pick any intervention, no matter how counterproductive, implausible, or just plain stupid, and you can probably find a fully-accredited MD somewhere who's evangelizing it from the rooftops.
Medical doctors are not scientists, or even engineers. They are more like highly-skilled technicians. NTTAWWT, but the MD degree by itself shouldn't bring individual doctors anywhere as much social and scientific credibility as it does. For most Americans, the best source of information on COVID has been, and remains, their public health authorities.
> "...the best source...has been, and remains, their public health authorities."
a contradictory conclusion, and somehow both falling for and denying the appeal to authority fallacy at the same time. you discount doctors being 'experts' but then claim another group of 'experts' being the right ones (with no justification, no less).
there is no shortcut when it comes to triangulating reality. all the data must be considered, not just your favored sources. otherwise, you will be biased and very likely incorrect (you shouldn't even have favored sources). note that the original article literally points out a bias/fallacy that public health officials have fallen prey to.
Public health authorites != some random "doctor" being interviewed or quoted by right-wing media. The authorities are more likely to be correct than an individual physician with a Twitter account, a bunch of junk-science citations, and an axe to grind.
It should be obvious that the burden of proof lies with the outlying opinion, but somehow, it never is.
> Public health authorites != some random "doctor" being interviewed or quoted by right-wing media.
Prasad is routinely interviewed & quoted by the "left-wing media". You are eager to fixate on the "wing" of the media coverage, but not engage with the argument being made.
Public health "authorities" are groups of people with opinions. Other people with expertise are no more or less qualified to have opinions, even if you don't agree with those opinions. If those opinions are backed by evidence and reason, and your opinions are backed by appeals to authority, then you lose.
> It should be obvious that the burden of proof lies with the outlying opinion
Close, but wrong. The burden of proof lies on the person advancing a hypothesis, whether that person is within the consensus or outside of it. Citing an authority does not excuse you from the burden of proof, any more than it excused the church in the time of Gallileo.
> If this pandemic has proven anything at all, it's that incompetent and/or corrupt doctors are a dime a dozen.
Not sure which side of the argument you are on, but it's funny, did you see how the death count for vaccinated people on the 22,000 pfizer study has been corrected from 17 to 24 people?
And the FDA has asked for 76 years to ongoingly release the safety data on the vaccine?
I'm vaccinated, but I'm super angry and worried about wtf is going on here.
What's certain is, yes: If this pandemic has proven anything, it's that there are incompetent and corrupt people EVERYWHERE on ALL SIDES.
In reality, the so-called "Public Health and Medical Professionals for Transparency" aren't interested in truth or transparency. They are just spamming the FDA with gratuitous FOIA requests in order to grind their political axe:
On a fundamental level the recommendation is the wrong way around as a matter of basic physics.
Filters work better under suction than pressure - because they are less likely to leak.
So why have a nonsensical system where everybody has to wear a mask properly all the time and change it regularly in the correct manner just to have any material effect, when an individual that is worried could just wear a better one that filters inbound properly and everybody gets to do what they want.
What's interesting about this is the psychology of why intelligent people have swallowed this. Do they believe the mask is filtering inbound when it isn't? Or is it entirely political - signalling membership of a group to others. Or is it that the perennially worried believe they should have the right to tell others what they can and can't do, when there is a perfectly reasonably 'live and let live' option available.
Why choose a position that divides society when there is one that brings people together?
I've always heard it as masks being more to protect others during the time where you're infectious but largely asymptomatic. At any rate, you can't prove you're uninfected easily - but masks are trivial to validate.
Why do you need to 'protect others' if their mask works inbound?
You have no idea whether you are 'protecting others' or just creating plastic waste for no good reason. Clearly masks are not trivial to validate given that there is no evidence they have any positive effect whatsoever in the real world. No deflection in rates can be seen from NPIs and the process leaks like crazy.
It's entirely a backward belief. Believing you are 'protecting others', yet doing nothing to protect yourself against the almost certain risk that other people won't be 'protecting others'.
None of it makes any sense in any logical analysis.
But there's another point the article is making: if mask wearing leads to people ignoring distancing because of a false sense that the mask provides them with strong enough protection that they can relax that, if this is observable how people act in aggregate, then maybe it does make sense overall not to have a mandate as a public health matter.
Anecdotally this is absolutely true. I know several people who wear masks while sitting in a car for long period of time with someone else. I know others who think going on jam packed public transport with a mask is basically safe. The least bad are the teachers who think when you spend an hour in a classroom with 30 people a mask will keep you safe.
Aerosol transmission.
It won't. In an hour the air will fill with the virus if someone is infected. The original virus apparently took 15 minutes to infect in a room. If delta is minimum 6x more infectious we are talking minutes.
By increasing air circulation, or meeting outside, we can reduce infections much more than if 30 people are wearing a mask inside a room for an hour.
To me it seemed more like it was because there was not a great enough supply of masks, so to avoid having the general population buy them all up but to save them for medical workers, this message was communicated.
I remember this being explicitly stated: please leave the masks for front line workers. In the US in the early days of the pandemic one item that kept reappearing in the news was the insufficiency of the PPE supply, including masks. The Trump administration was getting pounded on (outside of his friendly media) for the insufficiency of its efforts to remedy this. They were leaving it up to the states to duke it out among themselves. Supplies, including masks, were being horded and then resold at exorbitant prices. Jared was in the news for a shady deal relating to acquiring masks. There were news stories about people selling defective masks. I don't understand how this all seems to have dropped out of everyone's memory.
I assumed that we were not told to use masks here in the UK because there was a limited supply of them at the time and they didn't want that supply diverted from medical settings.
its very true. I worked in a research lab in health and it was unbearable being around those people.
'we can't do that, people will use it wrongly' 'we cant tell the people that, they might use the information wrongly.' on and on again.
Just one of many examples was a trauma center application that showed all the trauma centers in the US on a map. you could see the coverages for ambulance and helicopter. I put in a feature where one could see the distance to the closest trauma center, as well as get directions. I was asked to remove it because people might use the information incorrectly.
to me, the problem is much more broad than this article suggests. its not just one phenomenon. lying and hiding information is built into their way of thinking.
If you're going to publish information that people might rely upon, especially in an emergency, you're taking on the responsibility of maintaining the accuracy of that information, including possibly taking on the responsibility of ensuring stale data is retracted.
The greater the details, the greater the burden. People naturally make assumptions about credibility according to the depth and breadth of the information provided. If you're not prepared to make the commitment, then it's quite prudent not to publish so many details. If you don't publish it, then people can't mistake it for up-to-date, accurate, and/or comprehensive information, and they'll be more likely seek it out somewhere else or otherwise hedge their reliance. If you do publish and it's inaccurate, then you're misleading people and possibly redirecting them away from other, more reliable sources.
It's difficult to say without more details what the fundamental concerns in your case were. But note that the real, nuanced reasons for certain decisions aren't or can't always be adequately explained to employees. A lawyer or emergency services expert might give the sophisticated analysis, but by the time the directive makes it down to people implementing it the rationale is "because people are dumb". But in truth it's really more that people are trusting.
> If you're going to publish information that people might rely upon, especially in an emergency, you're taking on the responsibility of maintaining the accuracy of that information
That doesn't seem to work that way in most situations.
For instance there is a mandatory floor plan in all public buildings in case of emergency, and now with covid some do flow control by physically blocking entries/exits. These maps aren't updated to cross out blocked paths, and nobody seems to getting sued to outer space.
Gov sites are regularily broken, out of date, ridden with errors. I once needed to go to an clinic and used the GPS coordinates to go there, only to realize midway they were the town center coordinates and not the accurate building's coordinate. They still operate, I requested an update and it's not fixed.
Well, there is a different between blocking / limiting certain doors for regular use as entries / exits and physically blocking fire exits. Doing the first is absolutely fine, the later doesn't help with flow control anyway.
Yes, but not always in the way you expect. Because people tend to distrust government with money, they often tend to try and spend the least amount of money for software. Everyone who works in software knows that that often means that you get a shitty product.
On the other end of the spectrum is government being afraid to deliver a product that isn't 100% perfect. So they end up paying loads of money and delaying releases because of scope creep.
I've done a lot of consulting in government and these are two things I've seen there a lot.
Surely you can though! Isn't that what endangerment exists for (or is that bar too high?). I imagine if actual harm, or near harm, was required then it would be very difficult to enforce a lot standards.
A lot of enforcement comes from government authority and fines and what not, not lawsuits and not private lawsuits.
I mean, you're welcome to file a suit, but if you don't have a contract, and you don't have actual harm, and you don't have statuatory harm, expect your suit to be dismissed.
The idea that people should look at a map of hospitals in an emergency is pretty much what the article is about. It's a worry that people will do something stupid if information is available.
If you don't know dead cold where the trauma center is, you should be calling 911 (or equivalent), not trying to decide where to drive.
If you are in the middle of nowhere, you don't need to drive to the closest trauma center to improve the situation, drive to the nearest larger town/city. There will be a way of landing a helicopter there.
Just to play devils advocate, without knowing the exact details of the OP's product: you provide an electronic map, much like a subway map, of trauma centers with minimum necessary details, like only through streets and clearly labeled names which makes it effortless to plan, at a glance, the shortest route. Great. If they take what looks like the shortest route and hit road construction or traffic, they won't hesitate to analyze the situation on the spot and reroute if they believe it the better bet.
But now you add some helpful little details--a colored route from A to B with a label, "5 minutes drive time". Now they reach the obstruction. Will they immediately assess the situation as they see it, or will they believe that "5 minutes" already accounts for the time necessary to pass the obstruction, thus hesitating under the false belief that the electronic map is using hidden information?
EDIT: Note that this situation describes the error in the CDC's mask decision as discussed in the article. What the CDC should have said at the time was that it wasn't going to mandate masks because it lackedconfidence in its information regarding mask advocacy and efficacy. Instead what the CDC did was affirmatively tell people not to wear masks. If gave people too much detail and implied that it knew more than it really did. We can argue over whether the CDC should have known that masks were beneficial, but I think most can agree that they should have been more careful about giving false confidence eitherway. People aren't stupid, but they are easily misled, and once misled they'll continue rationalizing the direction they're headed. That describes not only how people responded to the CDC guidance but to the CDC itself--its false confidence in the poor 1960s-era aerosol experiments that claimed more than it actually proved.
Misleading information is poisonous. First rule: "do no harm". That's paramount over the responsibility to affirmatively help people.
Withholding information that is largely accurate but not perfect is not harmless.
Say someone is moving to a new city and wants housing that is close to high level medical care. It's useful if they are able to access information about where it is located.
part of the problem is that in med-speak things are often classified as "does good" "does nothing" "does bad" and by default new or untested things are never in "does good"
I mean,
until a few years ago there was no scientific evidence that parachutes helped with surviving jumping off a plane
What this article assumes is that people in control and in research 1-2 years ago "knew everything about covid" or knew what we know now. They didn't.
What we should assume is that 99% of people in general are morons and not specialists - just like you and me are not specialists and belong to the same 99% and can't comprehend these things and because they can't understand these things, they are also failing in explaining that to public. Explanation takes understanding and thinking. Government officials(including in health) does not do thinking - they only act according to instructions.
We more or less know right now what is going on and IMO it is still debatable if mandatory masks are long-term solution. What general public has forgotten is that eyes are as good open doors for covid infection(and so far only distancing, good sunny weather and relaxed unstressed healthy people has prevented spread of virus or they have getting through covid sickness without noticing it - without symptoms), not to mention that masks does not offer 100% protection, but more like 80%, not to mention that people are 100% unprotected when they have to eat or drink or if they are entering without spacesuit in highly infectious rooms. So, in short - it is easier to tell people to wear masks - but it would take a lot of explaining all iffs, where covid infection can be passed from one to another, so correct information would be that masks can reduce covid infections, but not prevent it fully.
Besides the main problem here is that covid is not deadly virus for healthy people, but it affects mainly people who are already living their last days. It just is mind bogling, that people in general have no idea how many people are dying every year and that that number is too big for what medical services were meant for.
As for seatbelts - some of the deaths in car crashes could be avoidable if seatbelts were not worn, as passenger might have been ejected out of car and could have a chance of surviving impact(if it is not a wall or other car, but grass or bush) after landing, instead of burning alive inside of crashed car. So, everything depends on situation and timing to receive that help where it is possible to help.
Those maps are there for the fire department, so they can check all rooms when they sweep a building. They're not stupid to use them for that purpose. Exit signs are for aiding egress. Personally, I use those maps to find the bathroom.
There will be a way of landing a helicopter there.
This isn't a huge issue in the countryside - this is one of the uses of medical helicopters, honestly. You are probably better off getting folks at the scene to help stablize you and allowing the helicopter to come there. That is, unless you were told to go somewhere else.
(I've nearly lost a tree for a medical helicopter when I lived by a overly dangerous curve: They decided to close the road and land there instead. They also help in rugged terrain).
A sub-10 mile ambulance trip can easily cost $1000 US if it's not covered by insurance. If you're already barely eeking out a living working paycheck to paycheck, that might be a bit too much to manage.
America does not have much compassion in healthcare, the fear of medical debt may outweigh the fear of death.
Absolutely agree. Knowing where a hospital is is a very useful information. Not everything requires emergency transport, does it? Not even in countries where emergency transport is covered by public health insurance. Knowing exactly what level of care, trauma and other, these hospitals are providing aren't really helpful in an emergency.
As a tangent, what really annoys me lately is Google Maps. For some very stupid reason Maps is not coming up with a destination of Covid test or vaccination centers, instead Maps is redirecting you to general search to get the latest news on Covid. There you can look up the address and manually navigate there. And even then it happened to me once the Maps refused to accept that destination. No idea what the reasoning behind that would be.
> Disagree. Just make it available with a clearly visible note saying it might not be updated, so verify once before using it for emergencies.
> People insist on making simple things too complicated.
Didn't you just make it more complicated here?
By adding a disclaimer? And at the same time presenting possibly outdated information? And requiring people to verify the information with another source?
While deep down knowing very well, that a lot, if not most, will not double check the information, before they end in an emergency?
And also, verifying for accuracy once does nothing, if the information becomes outdated, between verifying and the time of the emergency.
The simplest solution here, was what they actually did. They removed the information that was the source of the confusion.
> including possibly taking on the responsibility of ensuring stale data is retracted
SO much of the current covid conspiracy stuff relies on redacted studies. The thing is, the conspiracy theorists either think that they've been redacted because of "the man", or don't know how redaction works full stop.
I think another big part of it is, the conspiracy theorists only need one paper that agrees with them to instantly say the gazillions of papers that disagree with them are wrong. So even one redacted paper is more important to them than all other scholarship.
This article talks about their fear that masks would cause reckless behavior being a main reason they told everyone they were useless, but another one I've heard in interviews is they thought medical staff needed them more and the public could not be trusted not to hog them if they told the truth. Pretty clear that waffling was a total disaster with serious harmful effects.
Arg, so true. People that assume everybody is more stupid then them are the worst. I have friends (that sometimes are on the verge of not being friends) that always remind me what a huge responsibility a puppy is when you show them pictures of new family member, or that your mortgage is so high you can't travel anymore and you have to have priorities in life, "you have to be able to enjoy it too".
Assuming I'm to stupid to think for myself is the most insulting thing you can do to me. Sadly I still can't respond to this behavior properly, I get so worked up, it messes up my day. It even causes me to complain about it on HN.
Yes, and I think the whole concept is seriously dangerous. I hate it generally, because I hold truth is such an important ideal personally, but at a time where trust in democracy is dropping around much of the 'Western world', intentionally hiding information because you worry people will misuse it just throws fuel on the fire because it gives conspiracy nuts a 'grain of truth' to build their falsehoods on.
I think it's just so bad - when you have people making up crazy stuff about Government control (like the crazy stuff around vaccines being population control, injecting tracking microchips, the QAnon cult, etc. that are all getting massive), actually having real examples of the Government lying is basically the worst thing that you can have!
I used to work at a company that did HIV research ... the virologists that use to work there were losing their minds last year.
The "people will take stupid risks" if we give them protective measures was in full force, right down to Dr. Tam telling Canadians that we didn't need masks, that the public "wouldn't know how to use them correctly anyway" and just endanger ourselves even more, so save the masks for the medical profession.
At the time there was a severe shortage of even surgical masks, so it was a very good decision to ensure medical professionals have a plentiful supply. The panic/hoarding of masks would have endangered their lives in March and April of 2020. Note how the advice on mask wearing took a steep turn right around the time the supply issues were essentially resolved. Not a coincidence.
I have more than vivid memory of the situation - I took part of an effort to ship PPE to friends and family in Asia in January and I started to keep notes as soon as I realized that people are attempting to rewrite what happened.
By 02/02/2020 masks were no longer available in retail channels in the US. Not on Amazon, not in your local store, not at any price.
Retailers ware not competing with hospitals for mask allocations - they we simply cut out. There was even an article on Bloomberg which I can't find right now that talked about supply channels and why your Walgreens won't be stocking masks anytime soon.
The notion that we were told a noble white lie to help protect our health professionals was invented a few months later to whitewash the incredible incompetence of our health officials/administration at the time.
In Czech Republic we were much lower down the food chain when it came to masks, so there was no hope of getting them early on in the pandemic. So something novel happened - people were encouraged[0] to sew their own and wear them at all times. Over the course of a week or so we went from a country where mask-wearing was basically unheard of to everyone having their face covered when out in public. During that period (until ~September or so?) we frequently had the lowest number of daily cases-per-capita in Europe. Later the requirement for masks was removed altogether and all restrictions were relaxed ... then cases exploded to the point where we had the highest number in the world.
What I'm saying is - it looks like a bit of honesty and an encouragement for the general public to improvise face covering could have helped the USA and Canada despite the chronic lack of "real" PPE. The criminally negligent messaging around masks caused hesitation and doubt that was a gift to the covid deniers who to this day refer to that huge u-turn on masks.
>I took part of an effort to ship PPE to friends and family in Asia in January
Apropos, when the similar effort by the "patriotic Chinese emigrants" here got reported in press, one common angle was to present it as a hostile act by the Chinese state and also a failure of Finnish state of not restricting the PPE sales.
My cousin has a drywall business, they stopped being able to buy n95 masks AFTER Dr. Tam made her statements. Might have gone in a different order the US, but you could still get n95 masks in Home Depot in Canada when our top health officials were asking us not to buy them.
There was no shortage of t-shirts and even if wrapping a t-shirt around your head wasn't effective, at least it would have been logically consistent with the eventual messaging of "wear a better mask now that you can get them."
The experts decided to burn their own reputations for a short term benefit, and are paying the price now with vaccine hesitancy and growing ire towards experts.
Getting the wording slightly wrong? The US Surgeon General was quite clear:
> "Seriously people- STOP BUYING MASKS! They are NOT effective in preventing general public from catching #Coronavirus"
I don't think typing "NOT" is a slight error in wording. The message was deliberate, and it wasn't just the US Surgeon General either. All the center/center-left media, which is what I read, was echoing the same message. Fox News and Trump telling lies is par for the course, but I don't consider that a license for everybody else to start telling lies as well.
If there's an epidemic starting, then only a small number of people have the disease. Everyone wearing a mask would help, but if you have a limited number of masks, you want to focus them on people likely to have/catch the disease.
The masks worn by people without the disease would be ineffective or even counterproductive if health care professionals were missing PPE as a result.
> if health care professionals were missing PPE as a result
True, but "don't buy masks NOW because the health workers need them" is totally different than "don't buy masks because they are not effective for the general public and can actually be worse" - being either a terribly wrong idea (like the article defends) or outright lying to the public (if the message was told not because it was believed to be true, but as a roundabout way of being extra emphatic to avoid the public hoarding masks and causing PPE shortages for health workers).
Yes. I really got the impression that Dr. Tam and the other experts were throwing "civilians" under the bus to keep the n95 masks for the medical profession.
The criminal part is downplaying airborne transmission risks so your "no masks" story doesn't fall apart.
At one point, ER Docs and Nurses were wearing goggles, face shields, double masking (n95 + surgical masks) and experimenting with microwaving the n95s for reuse and Dr. Tam was STILL saying there was no proof it was airborne.
Being a Canadian, this particular incident gave me so much mistrust in our government. It woke me up to the fact that I am not being told the truth but that I am being manipulated. I haven’t trusted a single word from officials since then.
I don't think anything they said stopped people from trying to purchase masks. Certainly a majority of the population decided not to, but very quickly all masks that were available to the public were bought.
In the end they had to control the medical supply chain. It's a lot more work than lying to the public, but it actually works. Unfortunately lying lost the trust of the public and COVID became a highly political issue.
"The authorities were lying to us" is not a very reassuring take but it's more reassuring than the truth, that in enormous part they're incompetent, actively dangerous morons. See how the FDA banned KN95s, how the CDC stopped the Seattle Flu Study from testing for COVID, the CDC's banning non-CDC laboratories from testing for COVID while itself screwing up tests, the endless delays with approving things like fractional dosing, boosters, neither using the AZ vaccines nor giving them away. At least they didn't get in the way of Operation Warp Speed too much.
The bulk purchase, hoarding and exfiltration of masks, disinfectant and similar goods by Chinese nationals living abroad under direction of the party into the home country to the detriment of the domestic populations happened anyway.
We'll never know, but I wonder if the government had said, "masks are good, but please PLEASE do not try to buy them. the government is purchasing what supply we have to save our doctors." Perhaps with the honesty, the medical professionals would have gotten the supplies they needed AND we would have less distrust in US healthcare institutions. The public trust that was lost from that first lie is significant, and I believe it hampers vaccination efforts to this day.
Because they know that people, myself including, are selfish and will prioritize their own and their loved one's safety over faceless and impersonal "medical professionals". As illogical as that may be or inefficient from a group context.
It's such a blatant, apologies for the hyperbole: "you are plebs and tax cattle, and not as important as these special people here".
There's so much more they could have done, it's crazy that lying to the public is what they decided on. The media of course didn't help either, saying things like "Trump trying to fast-track vaccines could end up being worse than covid".
They weren't lying. They really believed what they were saying. They were idiots then and that should inform what you believe about them now and forevermore.
The freedom patriot trolls were spreading masks designs before they committed into increasing the pandemics levels.
That's the most difficult thing to accept. Those people were just contrarians, "freedom" (however stupid one may think their concept of it is) or "truth" were irrelevant.
I think you hit the nail on the head. They argue against something with their own kind of "wokeness", not caring if that something is true or makes sense.
"It’s an idea that ...posits that people adjust their behavior in response to perceived risk: the safer you feel, the more risks you’ll take."
regarding road guardrails, for example: "...proponents of the idea make a stronger claim: that guardrails cause so much reckless driving that any potential safety benefits of guardrails are offset or even reversed."
I don't think that quite saves a click. Yes, you've posted what the idea is, but completely cut out the entire point of the article (that the actual amount of risk compensation that happens is usually low, and policy based on the idea tends to be more harmful)...
Take the guardrail thing for example - you posted the arguments of proponents, but cut out the response where it goes through how the actual evidence shows it's not at all the case that guardrails increase risky behaviour!
Sorry, I thought that was implied by the negative framing of the headline, but maybe not.
The current headline is a bit clickbaity--I wish they'd give a preview of what the article is about (like the old days?) and if people are interested, they can read the whole thing.
> But whenever risk compensation has been subjected to empirical scrutiny, the results are usually ambiguous, or the hypothesis fails spectacularly. And when risk compensation does play a part in behavior, it tends to do so in small and specific ways...
> The question—for driver safety, sexual activity, or public health—isn’t whether some individuals change their behavior in response to perceived risk. It’s whether, at the population level, an intervention makes the world a safer and better place.
Just to make it clear how the article is arguing that "risk compensation" is generally a bogus concept.
Risk compensation was my excuse to not wear a helmet when I biked to work. My argument was that the false sense of security meant that I would bike more rashly increasing my chances of getting into an accident.
In reality, when I did wear a helmet, I did not bike more rashly. If anything, the helmet was a constant reminder of the dangers involved in city biking which meant I was possibly more alert than I would have been without it.
The one thing helmet laws seem to do that may be a public health risk, at least in cities with bike share systems, is suppress how many people ride. When you cannot ride a bike without a helmet, a good chunk of people will opt to take a car or walk instead of using a bike share.
To my knowledge, the number of cyclist collisions stays relatively constant with the number of cyclists: more cyclists mean around the same total number of collisions, which is fewer on a per trip basis. As a benefit, by acting as a natural barrier between deadly fast steel boxes and pedestrians, having a lot of cyclists also saves pedestrian lives.
IME the argument on bike helmets is a little different: it's not that requiring helmets will encourage riskier biking behaviour, it's that requiring helmets will shift people to drive instead (and that an extra car on the road is increasing danger to _others_). It may still be a bogus argument, but it's definitely distinct from the risk compensation argument given in the article.
On the road, especially as a bike user, your behaviour is not the most important factor. By far the biggest risk to you on the road are motorists. There is evidence [0] to show that motorists pass helmeted cyclists more closely and humanoids with long (feminine) hair less closely. Similarly, purely anecdotal (but may have been studied), those white lines they paint on the road and call "bike lanes" cause motorists to pass closer (they drive right up to the white line).
Coming from a country where we all have to wear helmets by law (Australia) I've personally not understood the risk compensation aspect as I never experiencing biking without a helmet.
However, I can understand the argument of it potentially reducing the number of people wanting to ride a bike. Especially for casual riding inner city or suburbs.
The day I realized the government and health officials are not telling me the full picture because they don’t trust me to act intelligently is when I completely stopped listening to their advice.
Which the officials created, not the intelligent individuals who don’t think it wise to follow advice that is likely not accurate and for unknown reasons.
I ignore and believe what makes sense based on the literature and a dose of common sense. Wear a mask, avoid large indoor gatherings, socially distance and ventilate are just obvious things to do for a respiratory virus and if the government and all health authorities say otherwise I don't care.
I’ve mostly decided to take normal precautions and not to live in fear. I’ve also decided to wait for more information before getting vaccinated. I work from home and have little risk of contracting the disease. I’m taking a break on social gatherings and travel for a few years and then I’ll see what I do.
I misread "taking a break on social gatherings and travel for a few years" as that you were going to stop seeing people and then go to travelling for a few years. My head inserted a comma.
From that I envisioned a cliche I've seen a lot where that fear comment always sits alongside someone who always talks in one-way or another about breaking the social contract of a community and mad-maxxing it across the country to find a "better place with similar people", thus the lone-wolf.
Apologies from a dylexic brain, and maybe one that should reflect on its prejudices.
When oral contraceptives were first approved by the FDA in 1960, critics at the time warned that “the foundations of contemporary sexual morality may be threatened” by the ensuing promiscuity
>> When oral contraceptives were first approved by the FDA in 1960, critics at the time warned that “the foundations of contemporary sexual morality may be threatened” by the ensuing promiscuity
> Were they wrong?
Yes. Totally and absolutely wrong. Practice based on fear of consequence is not morality. Weakening the affect of consequence changed exactly nobody's morality. Anyone who claims a morality that is followed only by being based on enforcement through physical harm is pretty messed up.
Promiscuity levels changed with the change in cost of the alternatives. Morality of people making those choices did not budge one iota.
The question only makes sense in the context of what those critics believed about morality. If you substitute your own beliefs on morality, then they weren't even wrong -- it's just a different question.
Morality is the way you act when nobody is watching and the consequences are all but non-existent.
I don't think driving more slowly to stay under the speed limit in an enforcement blitz is moral behavior. I think driving as safely as practicable for the safety of pedestrians when there is no enforcement (eg in a poor and corrupt country) might well be moral.
If you have different definition of what morality is, that's ok but there's not much to discuss.
Morality is impacted by perceived norms. Perceived norms are impacted by incentivization. Underage kids making non-nude porn en masse on MySpace would not fly in 2005. Thirst baiting is normal on tiktok today.
Again practice is impacted by perceived norms. If you thought it was constrained by morality and it changed through change of norms and incentives then you just found out it wasn't. You don't have to like that. I sure don't.
There is no fear of punishment for not bringing your shopping cart back. No fine or social stigma. Yet most civilized people bring back their cart. Except where there is visible moral decay around them. I don't subscribe to a nihilistic view that any moral principles that a group of people can give up on were never moral principles.
Which, if your observation is true, that shopping cart return is motivated by utilitarian incentive. "If most of us do it, things work better and most us do so it makes sense."
Disagree with that all you like, you might well be right. I claim whatever it is it's a long way from promiscuity increasing with a decline in consequence for sexual activity from saying anything about the morals of those who would have loved to fornicate but lacked opportunity prior. Or indeed those so easily swayed by the "everyone does it" argument and were making a virtue of their lack off reasonable opportunity. Reasonable people may disagree with that of course.
Usually this kind of thing is imposed morality which isn't individual morals. "I want everyone else to follow what I think is moral by making (sex/drugs/other thing I dislike) have dire consequences through policy because I can't convince _them_ to do the right thing because _they_ lack [my] morals."
So did every piece of technology that was widely adopted change behavior.
So what?
So there's a value judgement about whether that change in the behavior of others is a good thing. So "morality" which is where this came in.
You want to make cases about the pill adoption and STD prevalence getting worse, go right ahead. It is different data and a very different case to make. Also far from obvious which way it goes, fwiw.
> So did every piece of technology that was widely adopted change behavior.
>So what?
It sounds relevant if the pill was introduced and got legalized on the grounds that it would not cause that kind of change but e.g. only help married couples to plan their pregnancies.
Nope. The kind of online porn you’re referring to only became practical with widespread adoption of broadband Internet. That didn’t happen until the early/mid 2000s [1]. Meanwhile downward trends in teen sex started at least as far back as the early 90s [2]. The biggest change by far was massive declines in teenage pregnancy, births, and abortions [3].
> diet soda (what if people chug the stuff and it makes the obesity epidemic worse?).
Isn't that one true though? Anecdotally, since the introduction of the stuff Americans have only gotten fatter. It makes intuitive sense to me that artificial sugars also contribute to insulin resistance, increasing the risk of diabetes. And while for any X you can pretty easily find nutrition studies that say "X kills you" and "X makes you live longer", it's not too hard to find studies linking diet soda to obesity: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4498394/
I'd guess both, and my guess is part of the problem is fat people who think diet soda is an alternative to actually dieting. Which seems like the sort of risk compensation the article is talking about.
People who drink diet soda gain no more weight than people who drink regular soda.
It is true, however, that people who drink diet soda or regular soda gain more weight than those who don’t drink soda at all.
Turns out diet soda does not make things better from a weight loss perspective, but it doesn’t make thing a worse either, which negates risk compensation as a theory.
> and my guess is part of the problem is fat people who think diet soda is an alternative to actually dieting
Reality TV is essentially fake. Even the real parts, since by its nature it focuses on the strange, absurd, bizarre and unusual. It's not that these things don't exist, but if they were common, normal, or usual, they wouldn't be featured on reality TV.
The reasoning should be like this: "I found support for the idea that fat people think diet soda is a good alternative to dieting on reality TV, so this idea is probably uncommon, unusual and strange."
This seems like a case where things can be correlated without being causal.
In other words, you can choose to drink soda, and make other decisions that lead to obesity - the cause of both might be the same. (You might be hinting at that by saying they "drink soda because they are overweight" but I'd suggest that's inaccurate. As in, being overweight doesn't cause soda consumption!)
I forget where I read it, but the reasoning I heard for it is that your body still thinks the zero calorie sweeteners are sugar, so it will store more calories from the food you're eating because your body is compensating for the lack of calories in the "sugar". I've also heard that the causation is reversed though, and that obese people are more likely to drink diet soda because it's a low effort way to try and lose weight. I don't know which is true though, so I just try to stick to water or fruit/vegetable juice if I want some more flavor.
Insulin is the mechanism through which body fat is stored, and you are implying that zero calorie sweeteners trigger an insulin response, but this is not true. The mechanism is more related to too little time between meals and excessive volume of food intake per meal, both of which help maintain high insulin levels and subsequent weight gain. Zero calorie sweeteners seem to reinforce the desire to eat for pleasure.
If diet soda induced an insulin response, then anyone on a ketogenic diet or fasting who drank a lot of them could end up with hypoglycemia. I have never heard of this happening. I personally drink diet soda and energy drinks while fasting, including a few two week fasts, and have never had anything like hypoglycemia as a result.
I agree. I am asserting that they don't cause an insulin response, and something else must be responsible, perhaps a reinforced addiction to short times between meals.
Perhaps, but some research indicates that artificial sweeteners could be causing metabolic disorders. It's not clear yet whether there's a real causative effect.
It was emptied due to the swine flu response in 2009-10. The Obama administration included funding to replenish it in the 2011 budget, but that was rejected by Congress.
And did what with the stockpile of enough n95 masks for every citizen? Threw them all away?
Point is, just because at one point there existed a team called the "pandemic response team", doesn't mean we were at all prepared in the way that GP is suggesting, or even that they would have helped at all
All medical equipment has expiration dates, including masks. It's possible that a lot was thrown away instead of replaced once the pandemic response team was disbanded.
In this case, an expired stockpile is better than no stockpile (and close to as good as an unexpired stockpile). Those expired masks could have saved a lot of lives.
Expired stock would have been thrown away every year from 2017 until March 2020 and most likely would have been legally required since it is medical equipment. That is a consequence of cutting funds for future disasters.
There’s a publicly available playbook that lists in excruciating detail all the steps that should be taken.
In fact, for the most part, they include the steps that were taken, except if they were followed as in the playbook they would have been taken a lot earlier.
> Throughout the pandemic, each time a public safety measure arrives on the scene, some experts fret that the masses will simply use the newfound sense of security as license to behave recklessly, canceling out or even reversing any benefits of the safety measure.
The public did recklessly go out and panic buy toilet paper. I suspect the experts may have a point.
People didn't "feel an extra sense of security" and therefore buy lots of toilet paper (recklessly.) Rather, they felt a sense of insecurity about running out of toilet paper.
It's just a knee-jerk rationalization of conservative portion of our brains, fundamentally based on distrust in other people.
I have my own story: These days many trans people are coming out, and sex change operation is becoming more socially acceptable. I was, for a moment, worried that trans people might be deciding on a whim/fashion to permanently alter themselves. But then I realized I miscounted - the number of people with gender dysphoria will always be greater than number of people unhappy with the change. So I changed my mind on this - it's always worth to change if someone really desires to.
Ultimately, the idea that "other people will do it wrong" is a very anti-democratic sentiment.
And of course, behind it there is an anti-regulation economist from the Chicago school. God nows how many people these cultist have killed overall in the past 50 years…
So, the underlying concept is not that decision under uncertainty is risky and people tend to shy away from it?
Especially people that are trained to think long, hard and nuanced about problems before coming to a conclusion? Because their scientific reputation is at stake?
The coin their business is build around?
The prospect of (a)social/classic media lynch mob, be it on facebook or yellowpress doesn't make the alternative more attractive.
The mob side of the problem is much easier to understand.
It's just the little ham actor in their mind, acting out his temper tantrums on the stage he calls his mind.
"It's me, I must be right.
They tell me I have to change!?
That can't be, finally its me and therefore I know and therefore I'm right.
Beside I don't like to change, it hurts.
Okay, it's just inconvenient, but...but that hurts too, mum"
Who could or would argue with that?
Well, for the most part politicians.
Often leaders.
Seldom good and inspired leaders.
Wearing masks is annoying, they cost money and in the beginning of the pandemic, we simply didn't have them. So we find all sorts of excuses against masks. Same for seat belts, they cost money and people didn't want to be tied to their seats.
It is not so different from companies that prevent you to repair your devices because "you may hurt yourself" when in reality, they just want to sell you a new one or go through their own overpriced service.
It is not the only argument you can use. You can say that masks are bad for the environment, it is single use plastic after all, that they promote crime and make communication harder by concealing one's face, that it impairs breathing, which is mostly debunked but who cares.
It is the opposite of "think of the children". False sense of security is used when you have a safety that works but don't want, and "think of the children" is when you want it but it doesn't work.
1. Humans cannot always interact with their surroundings at 100% mental clarity. Stupid mistakes can and will be made even by the most careful and skilled person. Fool-proof or defensive design features are very well embraced by engineers and the results have been a resounding positive.
2. Some interventions are probably not as benign as people assume, and this could become a confounding factor when it comes to analysing the outcome. Some motorcycle helmets, for example, have been found to trap CO2 at concentrations known to have a negative cognitive effect.
I get the feeling that there's a virtue aspect here. In absence of seat-belts, birth control, and vaccines, safety is possible—if you are careful and prudent. Therefore, up to the point where such options are available, public health initiatives encourage and celebrate prudence and carefulness.
Once a work-around becomes available, where one can be just as safe with half the prudence, it feels like cheating: now all these careless people can be safe without any of the admirable virtue in being prudent and following rules. So those in charge resist giving the people an easy way out, because doing so represents a path towards loss of credibility of the authority institution, who is constantly advocating for virtue in the people.
I think this gives an interesting perspective on the recent discussions that I read here about eBikes and the fact that in The Netherlands we don't wear bike helmets.
The argument I saw online[1] was exactly the pitfall the article describes: "everybody will behave safer because cyclists are so obviously fragile".
There's a difference between "cyclists will take more risks (with their own lives) if they wear a helmet" and "drivers will take more risks (with cyclists' lives) if they see cyclists wearing a helmet".
And you're leaving out by far the most important argument, which is "people are less likely to cycle if they're required to wear helmets".
To continue that last thought, less cycling means more deaths via lost health benefits, more deaths via more car journeys and more deaths due to pollution.
The remaining cyclists being run over by the increased motor traffic is a vicious cycle it's hard to break out of.
There was a study that proved helmets were harmfull. It basically said that cycling has health benefits, and if helmets were compulsory less people will cycle. And more people would die from obesity and relevant healtu issues, than were saved by helmets.
There is no harm examining the law of unintended consequences and policy makers should do that more often in fact. As TFA makes clear through it's examples, a second or third order effect cost/benefit analysis should not be taken to the point of absurdity or inaction; but you should always remember that fixing something risks breaking something else in the process.
From a quick search, I think the Charles Murray quote is talking about perverse incentives and time preference rather than risk compensation. It's a weird choice.
Ok, so there were warnings that vaccines will lead to a false sense of security. And, guess what? Those warnings were right! One only has to take a look at the numbers in, say, Germany to see that the current wave of the pandemic is the worst yet, and vaccines contributed to that negatively on several levels:
- they gave the government a false sense of security, so they are only now reacting to the dramatic rise in Covid cases.
- vaccinated people can both get Covid (with the current Delta variant) and transmit it, they just don't get as sick as unvaccinated people. Still, restrictions were eased for vaccinated people as a motivational measure to get vaccinated, and now the virus is being transmitted from vaccinated person to vaccinated person until it finds an unvaccinated one.
- vaccination is actually impeding the measures that can be taken in the future: there is the argument that restricting the freedom of movement of a vaccinated person may be an undue breach of their constitutional rights, so there will be even more hesitation before extreme measures (lockdown).
I'm currently isolating at home with Covid despite being vaccinated, so please excuse me if I sound harsh. I'm actually glad that I am vaccinated, but I now see that the vaccine was more than just a bit hyped up by the authorities...
Are we really still yammering on about all this COVID-19 bullshit? We've got the vaccines, we've got antivirals on the way, and 85%+ of the US population has antibodies from either catching it or vaccinations. Move on. It really cracks me up to see people acting the same as they did during Week 1, like who are these people still cowering in their homes in fear who are more than eager to keep everyone else in a perpetual state of anxiety?
Maybe we ought to hand out some Xanax to the anxious folks driving all these fear-based policy decisions and constant churn of new articles that functionally try to weld the door shut on people's lives over a risk (at this point) that is far greater in the imagination than actual reality.
My glasses are always fogged up with my mask on. I've tried a few types, none seem to stop this, so I have to choose blurry without glasses, or foggy with them on.
At bicycle speeds with a mask I'd definitely want / need that helmet.
We've all learned about friends and family, which of them is fundamentally a coward to their core. If they haven't turned off their TV or started filtering out the shepherd's tone of fear mongering at this point, nothing would ever change their cowardice.
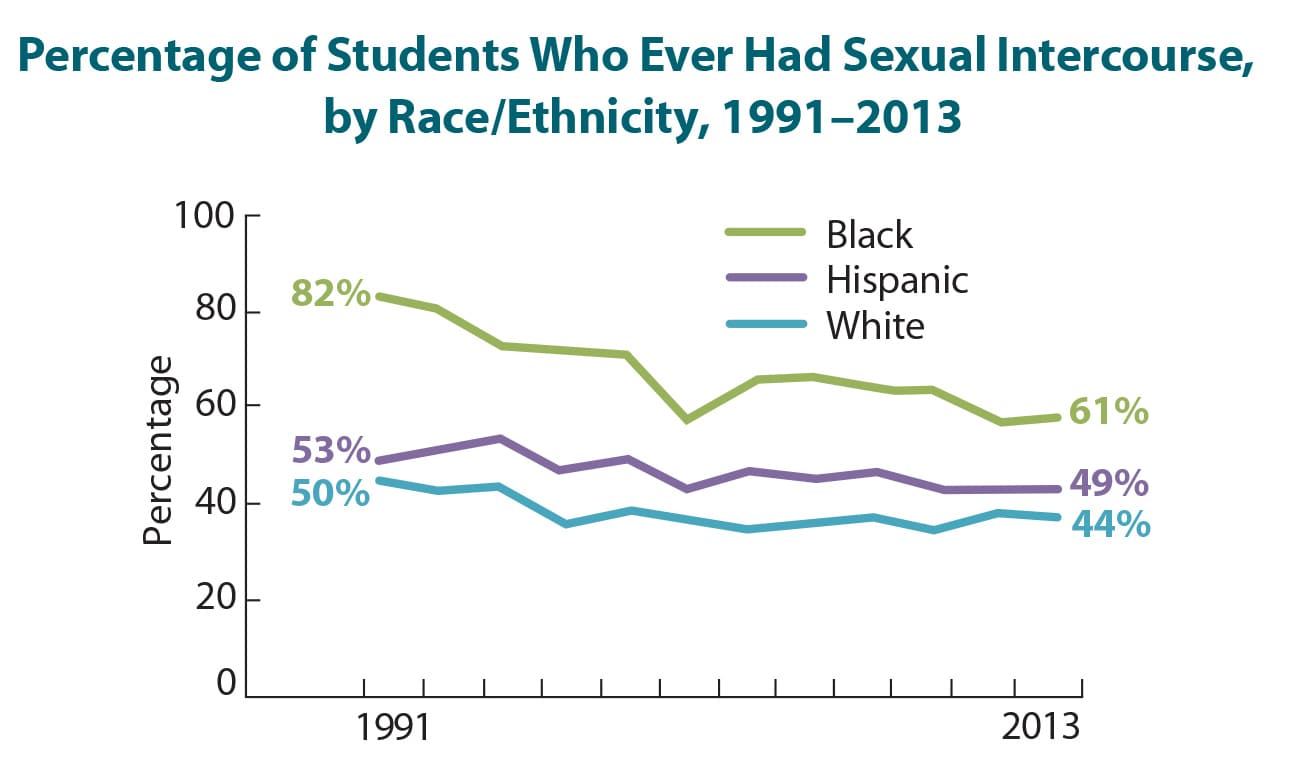{kind=link}
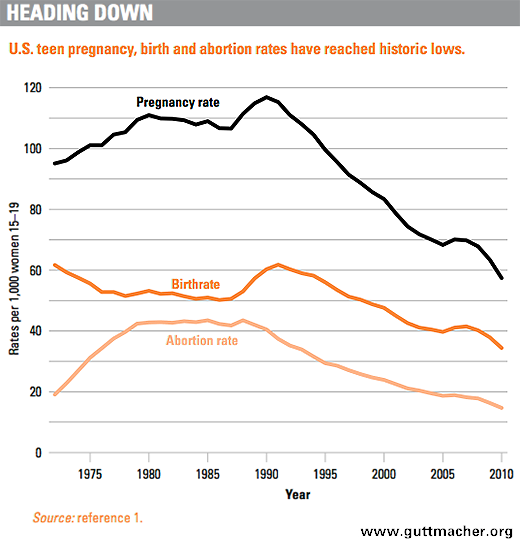{kind=link}
During the early stages of the pandemic, high ranking officials suggested we should not use masks because it was not yet "proven" the virus was transmitted via aerosols. And this was a catastrophic decision.
We always need to reason under uncertainty. The correct interpretation of the scientific method would have led to the conclusion that COVID was likely to be transmitted via aerosols (e.g. due to sequence similarity with other coronaviruses, which are known to be transmitted via aerosols) and imposing mandatory masks (because this is a very innocuous intervention).